
Brain metastases
A metastatic brain tumor (also known as brain metastasis or secondary brain tumor) is cancer that begins elsewhere in the body and spreads to the brain. The metastatic brain tumor usually contains the same type of cancer cells found at the primary cancer site. For example, cancer cells in the lung, breast, skin, colon or kidney can move into the brain through the bloodstream and cause a metastatic tumor. Brain metastases can be a single tumor or multiple tumors.
Metastatic brain tumors currently have the fastest growing rate of incidence of any tumor type. People are surviving cancer longer than ever before due to improved therapies. However, the primary cancer can continue to exist in the body and with time may recur in the brain as a metastatic brain tumor.
|
Incidence
- Metastatic brain tumors are the most common brain tumor in adults. The incidence of brain metastasis is estimated to be ten times higher than that of all primary brain tumors combined.
- The incidence begins to increase in those ages 45–64 years and is highest in people over 65 years of age. As people are living longer with their cancers, more of the population will develop metastases.
- The exact incidence of metastatic brain tumors is not known but is estimated between 200,000 and 300,000 people per year.
- Research indicates that approximately 80+% of metastatic brain tumors arise as multiple tumors within the brain and 10–20% arise as a single tumor.
- About 85% of metastatic lesions are located in the cerebrum and 15% are located in the cerebellum.
- Although melanoma spreads to the brain more commonly in males than in females, gender does not seem to play a role in the overall incidence of brain metastases.
- Skin cancer (melanoma), lung cancer and breast cancer are the most frequent to develop brain metastasis and account for 67%-80% of all cancers.
- Central nervous system (CNS) metastasis is rare in children and accounts for only 6% of CNS tumors in children(لینک به تومور مغزی کودکان) .
Diagnosis of Metastatic Brain Tumors

After a patient with cancer begins to experience neurological symptoms, a doctor will usually order a neurological exam and a brain scan (CT or MRI) that can detect tumors in the brain
The images from a brain scan will help your doctor learn:
- Size and number of tumors
- Exact location of the tumor(s) within the brain or spine
- Impact on nearby structures
Although scans provide the physician with a probable diagnosis, examination of a sample of tumor tissue (from surgery) to remove the tumor or from a biopsy) under a microscope confirms the exact pathologic diagnosis.
Another way a metastatic brain tumor is found is during the clinical trial process. Patients with cancer may be offered new therapies (i.e., clinical trials) that require brain imaging, which may incidentally discover brain metastases.
The metastatic brain tumor usually contains the same type of cancer cells found at the primary cancer site. For example, lung cancer metastasizes to the brain and forms lung cancer in the brain. However, recent research is suggesting that some tumors develop new genetic mutations in the primary tumor when they spread to the brain.
On the rare occasion that a metastatic tumor is diagnosed before the primary cancer site is found, tests to locate the primary cancer will follow.
Metastatic Brain Tumor Symptoms
The symptoms of a metastatic brain tumor are the same as those of a primary brain tumor, and are related to the location of the tumor within the brain. Headache and seizures are the two most common signs of a brain tumor. Disturbance in the way one thinks and processes thoughts (cognition) is another common symptom. Motor problems, such as weakness on one side of the body or an unbalanced walk, can be related to a tumor located in the part of the brain that controls these functions.
pecific Types of Metastases

LUNG CANCER METASTASIS TO THE BRAIN
- Most common type of brain metastases in both men and women.
- The brain tumor is often found before, at the same time or soon after the primary lung tumor (average six to nine months).
- Multiple brain metastases are common.
BREAST CANCER METASTASIS TO THE BRAIN
- The second most common type of brain metastases in women.
- Metastases tend to occur a few years after the breast cancer is found (average 2–21⁄2 years), but metastases at five or 10 years post treatment are not unusual.
- Generally found in younger and premenopausal women, as they tend to have more triple negative breast cancer.
- More common in women with triple negative or HER2/neu positive breast cancer.
- Two or more metastatic brain tumors are common.
MELANOMA METASTASIS TO THE BRAIN
- Second most common type of brain metastases in men.
- Metastases tend to occur several years after the primary melanoma.
- Multiple brain metastases are common.
- Metastatic melanoma tumors are rich with blood vessels that have a high tendency to bleed.
COLON/COLORECTAL METASTASIS TO THE BRAIN
- Metastases tend to occur a few years after the primary tumor is found.
- A single metastatic tumor is common.
KIDNEY/RENAL METASTASIS TO THE BRAIN
- Metastases tend to occur within a few years after the primary tumor.
- Single tumors are common.
- The metastatic tumor often contains blood vessels that have a high tendency to bleed.
Metastatic Brain Tumor Treatment
Once your scan shows a suspected brain tumor, your next step will be a consultation with specialists who focus on the brain and central nervous system, such as a:
- neurosurgeon (surgeon who operates on the brain and nervous system)
- neuro-oncologist (doctor who specializes in treating nervous system cancers)
- radiation oncologist (doctor who uses radiation to treat cancer)
Your care team should include a multidisciplinary group of health care professionals that help you make treatment decisions. The team will need to balance the treatment for the primary cancer site with the treatment for the metastatic brain tumor. They will look at your scans to determine if the tumor(s) can be surgically removed, or if other treatment options would be more reasonable for you.
Treatment decisions will take into account not only long term survival possibilities, but your quality of life during and after treatment, as well as cognition concerns. When planning your treatment, your doctors will take several factors into consideration.
- Your history of cancer
- The status of that cancer
- Your overall health
- Number and size of metastatic tumors
- Location of the metastatic tumor(s) within the brain or spine
- The tumor’s response to past therapy and its potential response to future treatment
The three main categories of treatments for metastatic brain tumors include surgery, radiationand medical therapy (chemotherapy, targeted therapy or immune-based therapy). Your doctor may suggest a combination of these therapies.
As in any disease, there are possible side effects from brain tumor treatment. Ask your doctor to explain these effects. He or she can also help you and your family balance the risks against the benefits of treatment.
WHOLE-BRAIN RADIATION
Whole-brain radiation is a common form of radiation for metastatic brain tumors, especially when multiple tumors (more than three) are present. The goal of this therapy is to treat both the tumors seen on the imaging scan plus the tumors that are too small to be visible. As a result, whole-brain radiation may be both preventive and therapeutic.
An important and common concern about whole-brain radiation is its possible impact on cognition and thinking, as a large section of the brain is effected by the radiation. Research focused in this area is ongoing.
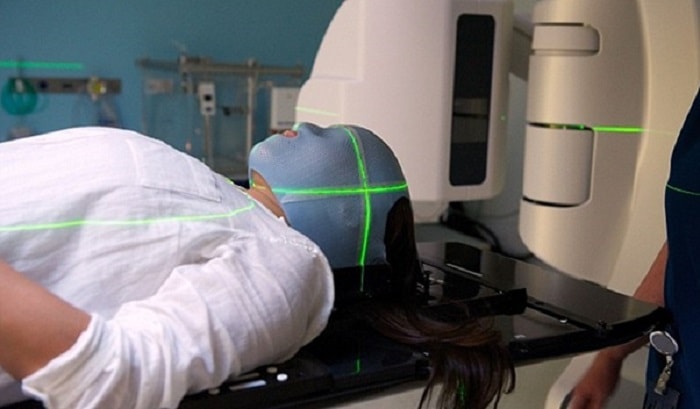
STEREOTACTIC RADIOSURGERY
Stereotactic radiosurgery (SRS) is a special form of radiation therapy. SRS, is a special type of radiation that allows precisely focused, high-dose x-ray beams to be delivered to a small, localized area of the brain. Because SRS focuses the beams more closely to the tumor than whole-brain radiation, it can deliver a higher, more effective dose of treatment to the tumor site.
Recent advances have made stereotactic radiosurgery an effective treatment option for some patients with brain metastases. Radiosurgery focuses high doses of radiation beams more closely to the tumor than whole brain radiation in an attempt to avoid and protect normal surrounding brain tissue. This approach is most commonly used in situations where there are fewer than three tumors and the tumors are relatively small (3 cm or less in diameter). Another consideration is whether the tumors are in eloquent regions of the brain, for example, speech and motor localized areas.
Radiosurgery can also be used to treat tumors that are not accessible with surgery, such as those deep within the brain. It may also be used for recurrences if whole-brain radiation was previously given, or as a local “boost” following whole-brain radiation. Examples of stereotactic radiosurgery machines are the LINAC radiosurgery, Gamma Knife or CyberKnife.
Surgery

Surgery may be more used when there is a single tumor and the cancer has not spread to other parts of the body. Some tumors may be completely removed. Tumors that are deep or that extend into brain tissue may be reduced in size (debulked). Surgery may reduce pressure and relieve symptoms in cases when the tumor cannot be removed.


